
Touch
Who doesn’t love the softness of an old t-shirt or the smoothness of a clean shave? Who actually enjoys having sand in their swimsuit? Our skin, the body’s largest organ, provides us with all sorts of information, such as whether something is smooth or bumpy, hot or cold, or even if it’s painful. Somatosensation—which includes our ability to sense touch, temperature and pain—transduces physical stimuli, such as fuzzy velvet or scalding water, into electrical potentials that can be processed by the brain.
Tactile sensation
Tactile stimuli—those that are associated with texture—are transduced by special receptors in the skin called mechanoreceptors. Just like photoreceptors in the eye and auditory hair cells in the ear, these allow for the conversion of one kind of energy into a form the brain can understand.
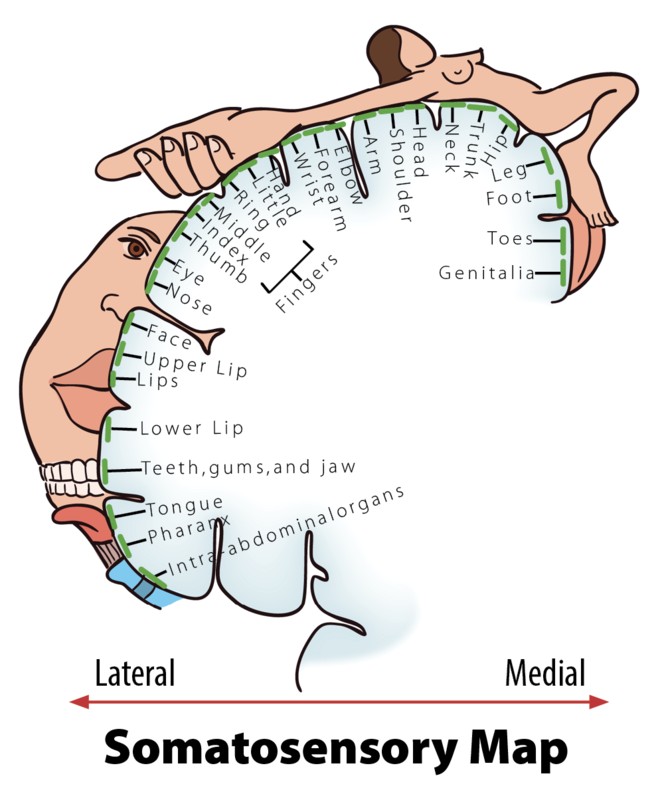
After tactile stimuli are converted by mechanoreceptors, information is sent through the thalamus to the primary somatosensory cortexfor further processing. This region of the cortex is organized in a somatotopic map where different regions are sized based on the sensitivity of specific parts on the opposite side of the body (Penfield & Rasmussen, 1950). Put simply, various areas of the skin, such as lips and fingertips, are more sensitive than others, such as shoulders or ankles. This sensitivity can be represented with the distorted proportions of the human body shown in Figure 5.
Pain
Most people, if asked, would love to get rid of pain (nociception), because the sensation is very unpleasant and doesn’t appear to have obvious value. But the perception of pain is our body’s way of sending us a signal that something is wrong and needs our attention. Without pain, how would we know when we are accidentally touching a hot stove, or that we should rest a strained arm after a hard workout?
Phantom limbs
Records of people experiencing phantom limbs after amputations have been around for centuries (Mitchell, 1871). As the name suggests, people with a phantom limb have the sensations such as itching seemingly coming from their missing limb. A phantom limb can also involve phantom limb pain, sometimes described as the muscles of the missing limb uncomfortably clenching. While the mechanisms underlying these phenomena are not fully understood, there is evidence to support that the damaged nerves from the amputation site are still sending information to the brain (Weinstein, 1998) and that the brain is reacting to this information (Ramachandran & Rogers-Ramachandran, 2000). There is an interesting treatment for the alleviation of phantom limb pain that works by tricking the brain, using a special mirror box to create a visual representation of the missing limb. The technique allows the patient to manipulate this representation into a more comfortable position (Ramachandran & Rogers-Ramachandran, 1996).
