
Studying the Human Brain
How do we know what the brain does? We have gathered knowledge about the functions of the brain from many different methods. Each method is useful for answering distinct types of questions, but the strongest evidence for a specific role or function of a particular brain area is converging evidence; that is, similar findings reported from multiple studies using different methods.
One of the first organized attempts to study the functions of the brain was phrenology, a popular field of study in the first half of the 19th century. Phrenologists assumed that various features of the brain, such as its uneven surface, are reflected on the skull; therefore, they attempted to correlate bumps and indentations of the skull with specific functions of the brain. Forexample, they would claim that a very artistic person has ridges on the head that vary in size and location from those of someone who is very good at spatial reasoning. Although the assumption that the skull reflects the underlying brain structure has been proven wrong, phrenology nonetheless significantly impacted current-day neuroscience and its thinking about the functions of the brain. That is, different parts of the brain are devoted to very specific functions that can be identified through scientific inquiry.
Neuroanatomy
Dissection of the brain, in either animals or cadavers, has been a critical tool of neuroscientists since 340 BC when Aristotle first published his dissections. Since then this method has advanced considerably with the discovery of various staining techniques that can highlight particular cells. Because the brain can be sliced very thinly, examined under the microscope, and particular cells highlighted, this method is especially useful for studying specific groups of neurons or small brain structures; that is, it has a very high spatial resolution. Dissections allow scientists to study changes in the brain that occur due to various diseases or experiences (e.g., exposure to drugs or brain injuries).
Virtual dissection studies with living humans are also conducted. Here, the brain is imaged using computerized axial tomography (CAT) or MRI scanners; they reveal with very high precision the various structures in the brain and can help detect changes in gray or white matter. These changes in the brain can then be correlated with behavior, such as performance on memory tests, and, therefore, implicate specific brain areas in certain cognitive functions.
Changing the Brain
Some researchers induce lesions or ablate (i.e., remove) parts of the brain in animals. If the animal’s behavior changes after the lesion, we can infer that the removed structure is important for that behavior. Lesions of human brains are studied in patient populations only; that is, patients who have lost a brain region due to a stroke or other injury, or who have had surgical removal of a structure to treat a particular disease (e.g., a callosotomy to control epilepsy, as in split-brain patients). From such case studies, we can infer brain function by measuring changes in the behavior of the patients before and after the lesion.
Because the brain works by generating electrical signals, it is also possible to change brain function with electrical stimulation. Transcranial magnetic stimulation (TMS) refers to a technique whereby a brief magnetic pulse is applied to the head that temporarily induces a weak electrical current in the brain. Although effects of TMS are sometimes referred to as temporary virtual lesions, it is more appropriate to describe the induced electricity as interference with neurons’ normal communication with each other. TMS allows very precise study of when events in the brain happen so it has a good temporal resolution, but its application is limited only to the surface of the cortex and cannot extend to deep areas of the brain.
Transcranial direct current stimulation (tDCS) is similar to TMS except that it uses electrical current directly, rather than inducing it with magnetic pulses, by placing small electrodes on the skull. A brain area is stimulated by a low current (equivalent to an AA battery) for a more extended period of time than TMS. When used in combination with cognitive training, tDCS has been shown to improve performance of many cognitive functions such as mathematical ability, memory, attention, and coordination (e.g., Brasil-Neto, 2012; Feng, Bowden, & Kautz, 2013; Kuo & Nitsche, 2012).
Neuroimaging
Neuroimaging tools are used to study the brain in action; that is, when it is engaged in a specific task. Positron emission tomography (PET) records blood flow in the brain. The PET scanner detects the radioactive substance that is injected into the bloodstream of the participant just before or while he or she is performing some task (e.g., adding numbers). Because active neuron populations require metabolites, more blood and hence more radioactive substance flows into those regions. PET scanners detect the injected radioactive substance in specific brain regions, allowing researchers to infer that those areas were active during the task. Functional magnetic resonance imaging (fMRI) also relies on blood flow in the brain. This method, however, measures the changes in oxygen levels in the blood and does not require any substance to be injected into the participant. Both of these tools have good spatial resolution (although not as precise as dissection studies), but because it takes at least several seconds for the blood to arrive to the active areas of the brain, PET and fMRI have poor temporal resolution; that is, they do not tell us very precisely when the activity occurred.
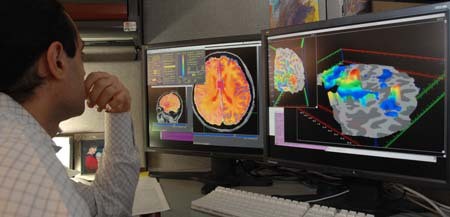
A researcher looking at the areas of activation in the brain of a study participant who had an fMRI scan – areas of brain activation are determined by the amount of blood flow to a certain area – the more blood flow, the higher the activation of that area of the brain. [Image: National Institute of Mental Health, CC0 Public Domain, https://goo.gl/m25gce]
Electroencephalography (EEG), on the other hand, measures the electrical activity of the brain, and therefore, it has a much greater temporal resolution (millisecond precision rather than seconds) than PET or fMRI. Like tDCS, electrodes are placed on the participant’s head when he or she is performing a task. In this case, however, many more electrodes are used, and they measure rather than produce activity. Because the electrical activity picked up at any particular electrode can be coming from anywhere in the brain, EEG has poor spatial resolution; that is, we have only a rough idea of which part of the brain generates the measured activity.
Diffuse optical imaging (DOI) can give researchers the best of both worlds: high spatial and temporal resolution, depending on how it is used. Here, one shines infrared light into the brain, and measures the light that comes back out. DOI relies on the fact that the properties of the light change when it passes through oxygenated blood, or when it encounters active neurons. Researchers can then infer from the properties of the collected light what regions in the brain were engaged by the task. When DOI is set up to detect changes in blood oxygen levels, the temporal resolution is low and comparable to PET or fMRI. However, when DOI is set up to directly detect active neurons, it has both high spatial and temporal resolution.
Because the spatial and temporal resolution of each tool varies, strongest evidence for what role a certain brain area serves comes from converging evidence. For example, we are more likely to believe that the hippocampal formation is involved in memory if multiple studies using a variety of tasks and different neuroimaging tools provide evidence for this hypothesis. The brain is a complex system, and only advances in brain research will show whether the brain can ever really understand itself.
